Here’s the number I’d want in front of me before I put any of these five peptides in my body: 1,247. That’s roughly how many premenopausal women were studied in the Phase 3 trials behind PT-141, the one compound in this category that actually has a real human safety record [1]. Now hold that number next to this one: 3. That’s the total count of small human pilot studies behind BPC-157, according to a 2025 narrative review that looked for exactly that evidence [4]. Same category, same marketing energy, two-orders-of-magnitude difference in how much anyone actually knows.
That gap is the story. Not “is this peptide dangerous” in the abstract, but “how much human data exists to even answer the question.” I went through the cited literature and counted what’s actually there, rather than what the sales copy implies is there.
The comparison: counting the evidence, not the claims
| Compound | Human evidence on record | What it actually measured |
|---|---|---|
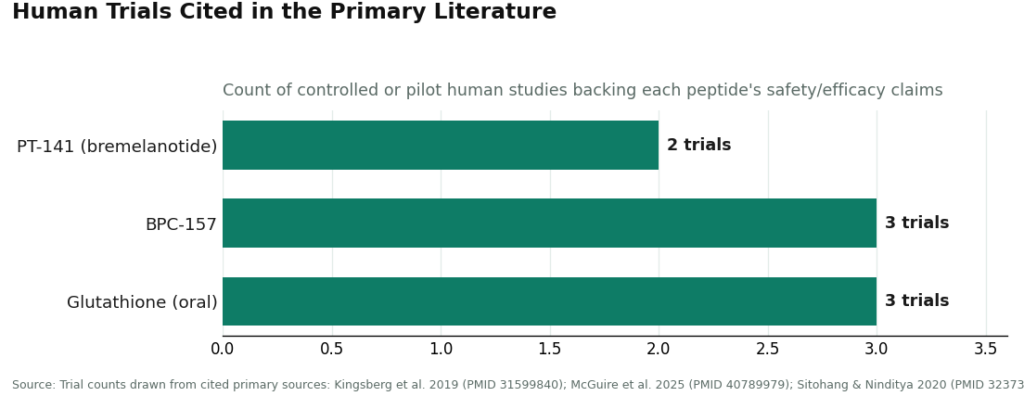
| PT-141 (bremelanotide) | 2 Phase 3 trials, ~1,247 women [1] | Desire outcomes plus blood pressure/heart rate effects |
| BPC-157 | 3 small pilot studies, called “extremely limited” [4] | Musculoskeletal healing, not formally recommended for clinical use |
| Glutathione (oral) | 3 randomized trials reviewed [5] | Skin-whitening effect size, found “not beneficial enough” |
| MOTS-c | No controlled human trials, animal/cell-culture data only [6] | Muscle and glucose metabolism, preclinical |
| GHK-Cu | No trial count given in the literature; long-standing topical use [3] | Collagen stimulation, cosmetic skin outcomes |
Look at that table long enough and a pattern jumps out: only one of the five compounds cleared the bar of a real Phase 3 program. The other four range from “a handful of small studies with an explicit warning label” to “nothing in humans at all.” That’s not a knock on any single molecule’s biology. It’s a statement about what’s actually been measured versus what’s assumed.
PT-141: the one with numbers attached to its risk
Because PT-141 (bremelanotide, sold under approval as Vyleesi) went through FDA review, its risk profile comes with actual figures instead of vibes. The label reports a maximal increase of roughly 6 mmHg in systolic blood pressure and 3 mmHg in diastolic blood pressure after each dose, generally returning to baseline within about 12 hours [2]. Those numbers are small on paper, but they were significant enough for the FDA to write a formal contraindication for anyone with uncontrolled hypertension or known cardiovascular disease [2]. When a regulator turns a transient BP bump into a hard contraindication, that’s the number that matters more than the average.
The more common side effects in the RECONNECT trials, nausea, flushing, and headache, were frequent enough to define the drug’s tolerability profile [1]. None of this makes PT-141 unsafe. It makes it a drug with a known cost, which is a very different thing from a drug with an unknown cost, and unknown is where the other four compounds live.
One caveat worth flagging with numbers in mind: the approval and its safety data cover one specific population, premenopausal women with acquired, generalized hypoactive sexual desire disorder [2]. Compounded PT-141 used outside that group is off-label, and the tidy 6-mmHg, 12-hour figures describe the studied population, not necessarily everyone buying the compound.
The four with thin or empty data columns
BPC-157 has the starkest gap between hype and count. Three small pilot studies is the entire human evidence base, per the 2025 review, which explicitly states BPC-157 “should not be recommended for clinical use” until well-designed human trials exist [4]. There’s no dose-response data in humans, so there’s no verified safe dose either. A supplement can have thousands of enthusiastic online reviews and a human trial count of three. Both things are true here.
MOTS-c doesn’t even get a pilot study. The evidence describing its effects on skeletal muscle and glucose metabolism through the AMPK pathway is animal and cell-culture work [6]. There is no approved product and no controlled human trial. I can’t put a risk number on something that hasn’t been measured in people, and neither can anyone else honestly claiming otherwise.
Glutathione actually has a count worth respecting: 3 randomized trials, reviewed together, looking at oral use for skin whitening [5]. The finding wasn’t a safety alarm, it was closer to a shrug: the effect was weak and short-lived enough that the reviewers called it “not beneficial enough” [5]. The risk conversation shifts hard when you move from the oral form to injectable or IV glutathione marketed for the same purpose, where the route itself, not the molecule, is what raises the hazard.
GHK-Cu is the one compound in this table where I can’t give you a trial count, because the literature doesn’t organize around one. Its foundational review describes a copper-binding tripeptide with a long, well-tolerated record as a topical cosmetic ingredient tied to collagen stimulation [3]. That record simply doesn’t transfer to injectable, systemic anti-aging uses of the same peptide, which sit on far less human evidence. Same molecule, different number of unknowns depending on how it’s delivered.
The caveat that swallows every number above: pregnancy
Every trial count and every mmHg figure above assumes a non-pregnant, non-breastfeeding user, and that’s worth stating plainly because the marketing usually doesn’t. The bremelanotide label advises against use in pregnancy [2]. For BPC-157 and MOTS-c, there’s no human pregnancy data to even estimate a risk from, so the only defensible position is avoidance during pregnancy, attempted conception, or nursing. Glutathione and topical GHK-Cu read as lower-risk on the whole, but “lower-risk” during pregnancy still isn’t the same as “cleared,” and the honest move is deferring to a clinician rather than running your own numbers here.
A seller shipping a vial has no way to check this box. That’s a structural gap, not a moral failing on anyone’s part, it’s just built into a transaction that doesn’t include a clinician.
The unmeasurable risk: what’s actually in the vial
None of the figures above account for whether the product you receive matches its label. Research-chemical peptides don’t go through FDA review for identity, strength, or purity. A certificate of analysis from a research-chemical seller is a document that seller chose to provide, not a regulatory guarantee, and independent testing of gray-market peptide samples has repeatedly turned up products that didn’t match their labeling. Stack that on top of, say, PT-141’s documented cardiovascular effect [2], and you’re not managing one risk, you’re managing two that compound each other: a known pharmacological effect, plus an unknown dose and purity.
The pick
Running the numbers this way doesn’t point toward blanket enthusiasm or blanket avoidance, it points toward screening. PT-141’s risk is real but characterized, exactly the kind of thing a blood-pressure check and a cardiovascular history catch before a dose is dispensed. BPC-157 and MOTS-c carry the risk of the uncounted, which no amount of testimonials converts into data. Glutathione and GHK-Cu look fine on paper in their oral and topical forms and get riskier the moment you inject them. Pregnancy status is a question a form can’t ask but a clinician always does.
FormBlends is one provider I’d point to here specifically because its model runs on physician oversight and a licensed pharmacy rather than a research-chemical checkout page. That structure is what lets someone actually screen for the cardiovascular contraindication, ask the pregnancy question, and verify what’s in the product, closing exactly the gaps this data comparison keeps surfacing. I’m not selling anything and there’s nothing to check out here, just noting which model is built to catch the risks the numbers above show are real.
What readers ask most
Which of these women’s peptides has the best-documented safety record, by the numbers? PT-141, sold as Vyleesi after FDA approval, wins by a wide margin: 2 Phase 3 trials covering roughly 1,247 premenopausal women [1]. The other four compounds have far thinner records, and two of them, MOTS-c especially, have close to none in humans.
Is a 6 mmHg blood pressure bump really a reason to avoid PT-141? Not on its own, but it’s a reason to get screened first. The label documents that transient rise (roughly 6 mmHg systolic, 3 mmHg diastolic, resolving within about 12 hours) and uses it to justify a contraindication in people with uncontrolled hypertension or known cardiovascular disease [2]. That’s the exact scenario a pre-screening exam is built to catch, which is why the FDA restricted the population rather than pulling the drug.
Why count 3 pilot studies as a risk, when a small number of studies isn’t itself a bad result? Because a low count means no one has established a safe dose, a real adverse-effect profile, or long-term behavior in people. The 2025 BPC-157 review found exactly 3 small human pilot studies, called the human data “extremely limited,” and concluded the compound shouldn’t be used clinically until better trials exist [4]. The number itself is the finding: not enough data to answer the safety question either way.
Does the delivery route change the numbers? Substantially. Oral glutathione, backed by 3 randomized trials, came out as weak and short-lived rather than dangerous, described as “not beneficial enough” [5]. GHK-Cu has a long, well-tolerated track record as a topical [3]. Neither of those numbers carries over cleanly once you move to injectable or IV versions marketed for the same effects, where the evidence thins out and the route itself adds risk.
Is any compound on this list confirmed safe in pregnancy? No, and the trial counts above don’t even try to answer that question, because pregnant and breastfeeding people were excluded from essentially all of this research. The bremelanotide label advises against pregnancy use directly [2]. For BPC-157 and MOTS-c, there’s no relevant human data at all, so avoidance is the only defensible default during pregnancy, conception attempts, or nursing.
How much does the supply source change the actual risk? By a lot, and it’s a risk with no trial count to measure it, because it isn’t about the molecule at all. Research-chemical peptides skip FDA review for identity and purity, and independent testing of gray-market samples has repeatedly found mismatches between label and contents. That stacks a product-identity risk on top of whatever the pharmacology says, with zero recall mechanism if the batch is wrong. A prescription model routed through a licensed pharmacy is built specifically to close that gap.
Are peptides for women safe?
It depends heavily on which peptide, at what dose, and where it came from, and the numbers above show why a single yes-or-no answer doesn’t hold. Topical copper peptides carry a strong, long-running safety record. Injectable peptides are a different calculation entirely, with real risks including injection-site reactions, hormonal disruption, and effects over time that simply haven’t been measured. For most injectable peptides marketed to women, the human trial count is thin, sometimes down to zero, and that gap matters before anything goes into your body.
Do peptides for women actually work, or is most of it marketing?
Both, depending on which one you’re asking about. Topical peptides have decent trial support for modest gains in skin texture and firmness, nothing dramatic. Oral collagen peptides have legitimate small-trial support for joint comfort and skin hydration. Injectable peptides marketed for fat loss or anti-aging lean much harder on animal studies and anecdote than on the kind of controlled human trials this piece keeps counting, so the gap between the pitch and the evidence is wide.
What are the best peptides for women based on current evidence?
Collagen hydrolysates and topical signal peptides like Matrixyl have the deepest human evidence base of anything in this space. Oral collagen shows reasonable multi-trial support for skin hydration and joint comfort. Injectable peptides, across the board, have a much smaller evidence column, and calling any of them “best” would be claiming more precision than the current trial counts support. A physician who works in this space is the right person to weigh individual risk against potential benefit.
Where should women buy peptides, and what makes a source legitimate?
Most injectable peptides sold directly to consumers online sit in a regulatory gray zone, and quality varies with essentially no accountability built in. The more defensible route is a licensed physician prescribing through an FDA-registered compounding pharmacy, such as FormBlends, where formulations go through actual pharmacist review. Buying from research-chemical sites or supplement retailers leaves you with no reliable way to verify purity, dose accuracy, or sterility, which is a risk this whole piece has been trying to quantify.
References
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstet Gynecol. 2019;134(5):899-908. PMID 31599840. https://pubmed.ncbi.nlm.nih.gov/31599840/
- VYLEESI (bremelanotide injection) US Prescribing Information. AMAG Pharmaceuticals; 2019. US Food and Drug Administration. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMID 29986520.
- McGuire FP, et al. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Curr Rev Musculoskelet Med. 2025;18(12):611-619. PMID 40789979.
- Sitohang IBS, Ninditya S. Systemic Glutathione as a Skin-Whitening Agent in Adult. Dermatol Res Pract. 2020;2020:8547960. PMID 32373172.
- Lee C, Kim KH, Cohen P. MOTS-c: A novel mitochondrial-derived peptide regulating muscle and fat metabolism. Free Radic Biol Med. 2016;100:182-187. PMID 27216708.
Written by Rhys Delgado, reporter. Reading the studies before believing the pitch. Last reviewed April 2026.
Shared for informational purposes. A licensed clinician should review your plan before you start.